
What is rotator cuff tendonitis?
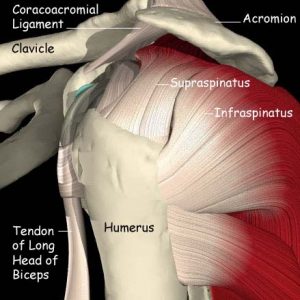 The rotator cuff consists of four muscles (subscapularis, infraspinatus, supraspinatus and teres minor). Rotator cuff tendonitis is secondary to injury to the supraspinatus and infraspinatus as they pass under the acromion or shoulder cap. Injury can be secondary to extrinsic (mechanical irritation) or intrinsic (primary muscular imbalance). In a normal individual, the space between the greater tuberosity and the undersurface of the acromion is approximately 6-7 mm. The thickness of the rotator cuff is approximately 5-6 mm. As one can see, there is little room for clearance in the normal individual. When the clearance diminishes, the rotator cuff gets pinched and rubbed beneath the anterolateral portion of the acromion. This may be due to a spur that develops under the anterolateral acromion and/or secondary to a poorly functioning rotator cuff. This irritation first begins as a bursitis. A bursa is a fluid filled sac that decreases friction between structures that must glide between each other. As the bursa becomes inflamed, it swells and becomes painful. If this continues unchecked, the tendon will become inflamed and swollen (bursitis). Finally, a chronic/irritated rotator cuff tendon may become so weakened that it tears.
The rotator cuff consists of four muscles (subscapularis, infraspinatus, supraspinatus and teres minor). Rotator cuff tendonitis is secondary to injury to the supraspinatus and infraspinatus as they pass under the acromion or shoulder cap. Injury can be secondary to extrinsic (mechanical irritation) or intrinsic (primary muscular imbalance). In a normal individual, the space between the greater tuberosity and the undersurface of the acromion is approximately 6-7 mm. The thickness of the rotator cuff is approximately 5-6 mm. As one can see, there is little room for clearance in the normal individual. When the clearance diminishes, the rotator cuff gets pinched and rubbed beneath the anterolateral portion of the acromion. This may be due to a spur that develops under the anterolateral acromion and/or secondary to a poorly functioning rotator cuff. This irritation first begins as a bursitis. A bursa is a fluid filled sac that decreases friction between structures that must glide between each other. As the bursa becomes inflamed, it swells and becomes painful. If this continues unchecked, the tendon will become inflamed and swollen (bursitis). Finally, a chronic/irritated rotator cuff tendon may become so weakened that it tears.
How is rotator cuff tendonitis diagnosed?
 Rotator cuff tendonitis usually causes pain over the anterolateral shoulder. Rotator cuff pain can be quite diffuse and patients often complain of pain from the shoulder to the back of the hand. Pain at night, with overhead activity, and while reaching for something in the back seat of the car are also common complaints.
Rotator cuff tendonitis usually causes pain over the anterolateral shoulder. Rotator cuff pain can be quite diffuse and patients often complain of pain from the shoulder to the back of the hand. Pain at night, with overhead activity, and while reaching for something in the back seat of the car are also common complaints.
On exam, the patient will often have a positive impingement sign. This test brings the rotator cuff directly beneath the acromion, thereby recreating the compression of the rotator cuff under the sub-acromial spur. Acromioclavicular joint pain, usually represented by pain directly over the AC joint, and cervical/neck pain, represented by pain and numbness from the neck to the hand distributed in a dermatome pattern, must also be ruled out. Also, if the patient has developed rotator cuff weakness, a rotator cuff tear must be ruled out.
How is rotator cuff tendonitis treated?
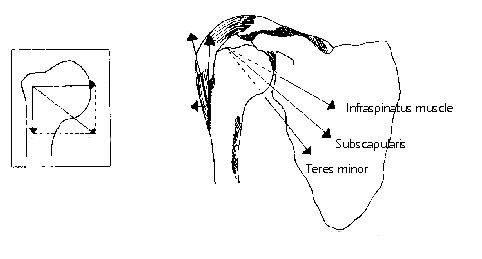
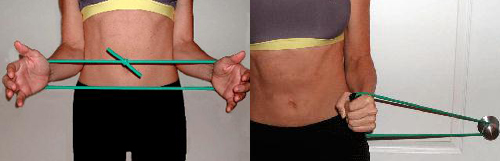
The goal of treatment of rotator cuff tendonitis is to increase the clearance for the rotator cuff beneath the acromion. This can be accomplished almost 70% of the time with a home rotator cuff strengthening program. A strong rotator cuff can increase the clearance under the acromion by a few millimeters. This depression effectively increases the clearance allowing the rotator cuff to heal. The key to rehabilitation is a proper program. The oblique muscles of the rotator cuff-the inferior portions of the infraspinatus, subscapularis and teres minor-attach at approximately 45 degrees to the humeral shaft. Therefore, a portion of these muscles’ job is to depress the humeral head during elevation. A proper home program that is performed three times a day with all exercises done on one’s the side is recommended.
The second approach to treatment is a sub-acromial injection. The injection is not placed into the tendon, but rather over it, and has an affect like placing salve on a sunburn. It decreases the swelling, thereby allowing more room for clearance. After approximately 24 to 48 hours, the patient resumes the home rotator cuff program.
If the patient fails conservative treatment, the next option is surgery. As long as a rotator cuff tear does not exist (diagnosed by an MRI or clinical weakness of the rotator cuff), we have the luxury of time and we can continue with conservative treatment. The surgery typically performed for rotator cuff tendonitis secondary to an anterolateral subacromial spur is an arthroscopic subacromial decompression. With the use of two small stab incisions and an arthroscope, the anterior spur is removed from the undersurface of the acromion, thereby increasing clearance for the rotator cuff. The surgery is performed as an outpatient and recovery is usually in approximately 6 weeks.
What if my rotator cuff is torn?
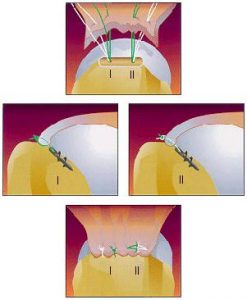
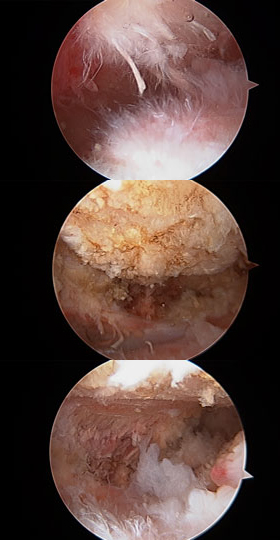 A torn rotator will not heal on its own. If the patient elects not to have the rotator cuff repaired, they must realize that the tear can extend and worsen. A strengthening program is not recommended but a physical therapy program to gain motion may be recommended. The surgery for a torn rotator cuff is initially performed arthroscopic. First, the spur is removed with a high-speed burr. Next, the tear is assessed for size, location and amount of retraction. If appropriate, the tear is repaired all-arthroscopically with the use of high tensile suture and small titanium anchors to reattach the tendon to the bone. Occasionally, a small (3 cm) incision is created to assist with the repair.
A torn rotator will not heal on its own. If the patient elects not to have the rotator cuff repaired, they must realize that the tear can extend and worsen. A strengthening program is not recommended but a physical therapy program to gain motion may be recommended. The surgery for a torn rotator cuff is initially performed arthroscopic. First, the spur is removed with a high-speed burr. Next, the tear is assessed for size, location and amount of retraction. If appropriate, the tear is repaired all-arthroscopically with the use of high tensile suture and small titanium anchors to reattach the tendon to the bone. Occasionally, a small (3 cm) incision is created to assist with the repair.
The surgery is performed as an outpatient. A sling is used for the first 24 hours and then is discarded. Physical therapy will begin approximately 1 week after surgery. It is stressed that full passive motion is allowed and important after a rotator cuff repair. This does not mean the patient can actively lift their arm, but rather, with the assistance of a therapist or their other arm, they should begin to regain full passive motion. The patient may perform “toes to nose” activities. This includes self-feeding, washing one’s face and buttoning one’s clothes.
A rotator cuff heals at approximately 10% – 15% per month. Whether you pitch for the Chicago Cubs or are an 80 year-old golfer, the rotator cuff will not be completely healed for 9 to 12 months. Generally, at 6 weeks post-op we begin a gradual strengthening program. Even at 3 months, the rotator cuff is only 30% – 45% healed but some light lifting is allowed.
How well do rotator cuff repairs do?
 In one study, 94% and 85% of patients in the small (< 1 cm) and medium (1–3 cm) tear groups, respectively, rated the status of their shoulder after surgery as either excellent or satisfactory. In contrast, results were excellent or satisfactory in 74% of patients in the large (3–5 cm) tear group, and in 27% of patients in the massive (> 5 cm) tear group. Re-tear, or failure to heal, for rotator cuff repairs as determined by MRI is 20% to 39%. For tears > 2 cm, the re-tear rate at 2 years is even higher (41–94%). Outcomes showed major initial improvement at 12 months despite these results, although there appears to be some deterioration thereafter. The bottom line is that rotator cuff repairs tend to fail as the tears become larger. A re-tear does not necessarily mean that you are going to have a bad outcome.
In one study, 94% and 85% of patients in the small (< 1 cm) and medium (1–3 cm) tear groups, respectively, rated the status of their shoulder after surgery as either excellent or satisfactory. In contrast, results were excellent or satisfactory in 74% of patients in the large (3–5 cm) tear group, and in 27% of patients in the massive (> 5 cm) tear group. Re-tear, or failure to heal, for rotator cuff repairs as determined by MRI is 20% to 39%. For tears > 2 cm, the re-tear rate at 2 years is even higher (41–94%). Outcomes showed major initial improvement at 12 months despite these results, although there appears to be some deterioration thereafter. The bottom line is that rotator cuff repairs tend to fail as the tears become larger. A re-tear does not necessarily mean that you are going to have a bad outcome.