
What is Chondromalacia Patellae?
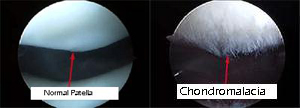
The term chondromalacia patella refers specifically to a pathological condition resulting in structural changes in the cartilage surface of the kneecap. Literally, “chondromalacia” means cartilage (chondro) softening (malacia). These changes may be as mild as softening and discoloration of the normally firm, white glistening surface. If the process continues, fissuring and fraying may occur, with the more advanced stages resulting in full thickness cartilage loss with exposure of the underlying bone. The process may be localized to one small area or it may involve the entire surface of the patella. Because of this variability in the degree of cartilage damage, the symptoms experienced by patients with chondromalacia may vary.
The patella aids the quadriceps muscle in extending the knee by improving its mechanical advantage. The articular surface of the patella is the thickest in the body (four to six millimeters). Walking on level ground exerts a patellofemoral force equivalent to one-half the body weight, climbing stairs between 3-8 times the body weight, and rising from a full squat can generate forces eight times the body weight.
What causes chondromalacia?
Although chondromalacia may develop following an acute injury to the knee (direct blow, fracture, or dislocation of the patella), more commonly, it has an insidious onset not specifically related to any one traumatic event. Any anatomical variation that results in “mal tracking” of the patella in the femoral groove during knee motion may expose the cartilage to larger loads than it can withstand resulting in abnormal wear. Predisposing factors include anatomical variations in patellofemoral groove, tight supporting structures, rotational malalignment of lower extremity (traumatic or developmental), or altered test alignments.
Who gets chondromalacia?
Chondromalacia is somewhat more common in women than men and is seen most frequently during the adolescent and early adult years, but may occur at any age. Most commonly, it is seen in females between the ages of 15 to 30 years. Activities that require a significant amount of kneeling, squatting, and stair climbing are commonly associated. In runners, increased mileage or hilly terrain may bring on the symptoms of chondromalacia.
What are the symptoms?
Although the symptoms vary somewhat, there is generally a dull aching pain across the front of the knee during or, more commonly, after an aggravating activity. With symptomatic episodes there may be a mild puffiness or feeling of fullness about the knee. There is often a noticeable “cracking” or “popping” with knee motion. Prolonged periods of sitting often result in an aching stiffness. Squatting, climbing stairs and, in particular, going downstairs provoke knee pain. The pain results from increased pressure on the bone under the area of abnormal cartilage. Irritation of the lining of the knee joint by particles of cartilage debris produces swelling and inflammatory pain.
How is chondromalacia diagnosed?
- The diagnosis is clinical and based upon the patient’s symptoms and examination of the symptomatic knee.
- While x-rays may be helpful in demonstrating anatomic variations associated with chondromalacia, they do not show the early changes taking place within the cartilage surface of the patella.
- Arthroscopy is rarely necessary to confirm the diagnosis. Occasionally an MRI, CT scan, or bone scan will be obtained to further evaluate the knee.
What is the prognosis?
Although chondromalacia does represent a mild form of arthritis, rarely does it result in severe, permanent damage to the knee. Symptoms fluctuate, related to patient activity. Treatment is aimed at reducing the frequency and severity of painful episodes and possibly eliminating the symptoms.
What is the treatment for chondromalacia?
One way to reduce the symptoms of chondromalacia is to avoid or modify those activities which aggravate the condition. A specific exercise program stressing quadriceps muscle and hamstring muscle stretching and strengthening often reduces the symptoms dramatically. Icing the knee after aggravating activities and occasional use of aspirin or other anti-inflammatory medication may also be helpful. A patella stabilizing brace may be beneficial in those individuals in whom patella maltracking is contributing to the condition.
Swimming is generally the most well tolerated fitness activity. In choosing a fitness program, one should use pain and swelling as a guide. Other physical therapy techniques include McConnell taping, which helps correct tight lateral structures.
Despite a conservative treatment program, a small percentage of patients with chondromalacia will continue to experience significant knee pain and disability. Surgery is sometimes elected in these individuals. A variety of surgical procedures that involve smoothing down the cartilage surface of the patella and/or realigning the quadriceps-patella complex are available.
These procedures are done arthroscopically although occasionally they require open surgical technique. In very rare instances it may be decided to completely remove the patella to alleviate the pain. In general, however, surgery for chondromalacia should be considered only after all other treatment methods have failed.
Clinical features:
- Anterior knee pain
- It occurs in women more than men
- Pain associated with going downstairs
- Crepitus
Treatment:
- The patient must take steps to avoid aggravating activities
- Physical therapy program to strengthen and stretch quadriceps and hamstrings
- Judicious use of NSAIDs
- Rarely operative intervention
Can you replace my kneecap?
Yes.
The patellofemoral replacement is a surgical method for the treatment of localized cartilage lesions in the patellofemoral joint (knee cap) that have failed conservative measures. The implant can be used with or without a patellar (knee cap) resurfacing product. The HemiCAP® (Arthrosurface) system is intended to provide an effective interim means for managing pain and disability in the middle-aged patient until a total joint replacement treatment option becomes more necessary, and is part of a clinical treatment strategy to help avoid early-age-revision scenarios. The implants and instruments are designed to remove a minimal amount of bone stock, preserve functional structures and tissues, and allow for an uncomplicated removal in the event of revision. This system is comprised of three elements; a three-dimensional mapping technology, a set of instruments to map and prepare the damaged area and a cobalt-chrome and titanium implant.
Early reports regarding PFJ replacement have been mixed. Revision rates have been shown to be between 4.2 to 9.9% with an overall satisfaction of 80%. The higher revision rate may be due to the fact that the procedure is performed on younger patients and the procedure is simpler that a total knee revision.
Summary:
Chondromalacia is a condition involving the cartilage surface of the kneecap. It can become symptomatic from a variety of causes. Usually, an aggravating activity can be identified. It rarely results in permanent disability. Conservative treatment including activity modification, a well-designed exercise program, selective use of ice, bracing and anti-inflammatory medication is usually successful in its treatment. Occasionally, surgery is elected to help relieve the symptoms of chondromalacia.