
How does arthritis destroy the knee?
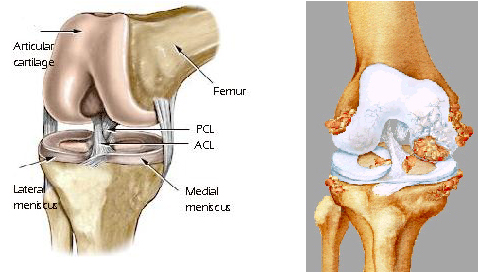
The ends of the femur (thighbone), tibia (shinbone) and the back of the patella (kneecap) form the knee joint. They are covered with a thin, smooth, glistening material called hyaline cartilage. It is the knee hyaline and meniscal cartilage that cushion the joint and absorb shock. Normally, this cartilage is lubricated by a few drops of specialized joint fluid. The arthritic knee may produce increased amounts of fluid, thus the name “water on the knee.” Cartilage has poor healing capabilities, and once it is damaged, it no longer provides cushioning. As it wears away, bone becomes exposed. Bone surfaces rubbing against each other can cause significant pain.
How do we treat arthritis without surgery?
Unfortunately, there is no cure for arthritis. Procedures such as cartilage transplant are not indicated for the person with a degenerative knee. They are generally used on the young athlete that has a small injury to their articular cartilage. Our initial approach is the alleviation of symptoms with conservative measures (oral medications, injections, activity modifications). All anti-inflammatory medications (NSAIDS, Advil, Aleve, Celebrex) have about the same effectiveness and only improve symptoms; they do not change the progression of the arthritis. Occasionally we will recommend an injection of an anti-inflammatory steroid into the knee joint. These injections are generally safe and well-tolerated and may be repeated every three months if found effective (4 or more times per year). Another type of injection is Synvisc (hyaluronic acid). This is a normal material found in the knee joint fluid, although in abnormal amounts in abnormal amounts in the arthritic knee. By injecting this medicine, the knee begins to produce more normal joint fluid. This is an expensive series of three injections that we have found to work approximately 50% of the time (less than 40% of the time in patients with advanced arthritis).
One may also control arthritis with activity modification. You can think that a degenerative knee is like having a tire with 50,000 miles of wear on it. One should continue to maintain a fit lifestyle, but an effort should be made to perform more unweighted activities. The best activity for your knee is pool aerobics. The next best activities are a stationary bike, recumbent bike, and elliptical trainer. Walking and treadmill machines are better than running. One should save higher impact activities for things that one really enjoys doing.
When should I have surgery?
There are surgical procedures for a degenerative knee other than a knee replacement. Occasionally, we will perform a knee scope to clean out debris and thereby decrease the soreness and swelling in the knee. This has variable results and the benefit is rarely sustained past one year. Other surgeries include unicompartmental knee replacement (replacing only the inner or outer portion of the knee) or an osteotomy (realigning the knee by cutting the femur or tibia.) These procedures are indicated in select patients.
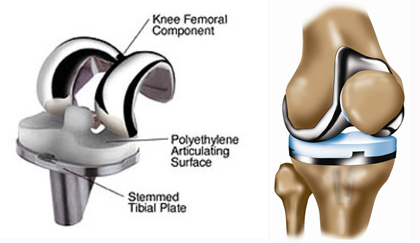
The main indication for total knee replacement is arthritis of the knee accompanied by considerable pain and loss of function that does not respond to conservative treatment. The decision to proceed with surgery is ultimately up to the patient. Arthritis of the knee is not a malignant condition and is not life threatening and quality of life is the main consideration. When you feel that you are living your life around your knee and your symptoms prevent you from living your life the way you wish, consideration to a knee replacement should be given.