
The thrower’s paradox.
 The thrower’s shoulder must be lax enough to allow excessive external rotation, but stable enough to prevent symptomatic humeral head subluxations, thus requiring a delicate balance between mobility and functional stability. We refer to this as the “thrower’s paradox.” This balance is frequently compromised, which leads to injury.
The thrower’s shoulder must be lax enough to allow excessive external rotation, but stable enough to prevent symptomatic humeral head subluxations, thus requiring a delicate balance between mobility and functional stability. We refer to this as the “thrower’s paradox.” This balance is frequently compromised, which leads to injury.
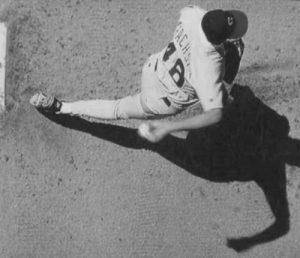
The overhand throwing motion occurs in six phases. Although many other movements have been studied (such as the volleyball spike, golf swing, and tennis serve), there are enough parallels between movements that the overhand throw serves as the most commonly used model. The goal of the motion is to sequentially develop a package of potential energy that is then converted to kinetic energy that can be imparted to the ball in an efficient and fluid manner. Quite remarkably, shoulder loads are minimal as the arm rotates internally at velocities greater than 7000 deg/sec.
The entire throwing motion takes less than 2 seconds. The wind-up and cocking phases require approximately 1.5 seconds. The acceleration phase takes approximately 0.05 seconds, and the deceleration and follow-through phases take approximately 0.35 seconds. The deceleration phase of throwing is the most violent phase and a contributor to GIRD.
What is Glenohumeral Internal Rotation Deficit- GIRD?
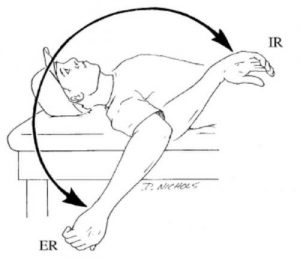 The reason for this altered range of motion is not clear, but it is believed to be a natural adaptation that develops in all throwers. Theories related to external rotation gain and GIRD include the presence of subtle microtrauma to the static and dynamic restraints of the glenohumeral joint from repetitive overhead throwing, contracture of the posteroinferior joint capsule, and osseous adaptation of the humerus. Despite the apparent alterations in the amount of rotation, the amount of total humeral rotation range of motion available in the throwing limb typically does not differ from that of the uninvolved limb. Range of motion alterations can become problematic in the throwing shoulder when the amount of glenohumeral internal rotation loss exceeds any gain in external rotation. This condition is a true internal rotation deficit from the total humeral rotation range of motion. The loss of internal rotation is believed to result from contracture and thickening of the posteroinferior portion of the glenohumeral joint capsule, which occurs from the repetitive microtrauma imparted during the deceleration phase of the throwing motion. A review of the disabled throwing shoulder, reported that arthroscopic findings in throwers who exhibit GIRD show a severely contracted and thickened posteroinferior recess in the posterior band of the inferior glenohumeral ligament.
The reason for this altered range of motion is not clear, but it is believed to be a natural adaptation that develops in all throwers. Theories related to external rotation gain and GIRD include the presence of subtle microtrauma to the static and dynamic restraints of the glenohumeral joint from repetitive overhead throwing, contracture of the posteroinferior joint capsule, and osseous adaptation of the humerus. Despite the apparent alterations in the amount of rotation, the amount of total humeral rotation range of motion available in the throwing limb typically does not differ from that of the uninvolved limb. Range of motion alterations can become problematic in the throwing shoulder when the amount of glenohumeral internal rotation loss exceeds any gain in external rotation. This condition is a true internal rotation deficit from the total humeral rotation range of motion. The loss of internal rotation is believed to result from contracture and thickening of the posteroinferior portion of the glenohumeral joint capsule, which occurs from the repetitive microtrauma imparted during the deceleration phase of the throwing motion. A review of the disabled throwing shoulder, reported that arthroscopic findings in throwers who exhibit GIRD show a severely contracted and thickened posteroinferior recess in the posterior band of the inferior glenohumeral ligament.
What injuries happen with GIRD?
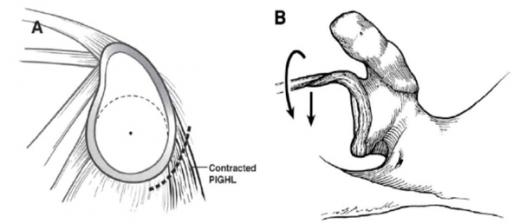
When the posterior capsule becomes tightened, the shoulder loses internal rotation. We used to believe that throwers used to develop “microinstability” to the front of the shoulder and required surgery to stabilize this looseness. We now feel that it is the tightness of the posterior shoulder (PIGHL, picture A) that causes damage to the rotator cuff and biceps tendon (picture B).
How is GIRD treated?
We believe that 90% of all throwers with symptomatic GIRD and posterior shoulder tightness will respond positively to a posteroinferior capsular stretching program. The program is a set of carefully designed stretches that selectively stretch different parts of the posterior capsule. These stretches need to be incorporated into one’s daily routine. An athlete that is a responder will usually gain 10 degrees of internal rotation within the first week. Only 10% of athletes will go on to require surgical intervention. Surgery often requires a SLAP repair with a posterior capsular release.
